The study (Healthcare integration) prepared in the frames of this subproject can be downloaded by clocking on the picture below (in Hungarian).

Results of the subproject were summarized in the following points. Click on the text for details.
Objective of the subproject
During the Legal Accessibility project, implemented in 2016, cross-border integration of health care services was identified as a priority topic, because numerous different questions emerged in the domain of this topic at the stakeholder workshops, and whose legal background is very complex and fair-reaching. The identified legal and administrative obstacles principally gathered around two topics, namely cross-border movement of patients and cross-border emergency activity. During the planning of the project in 2017, cross-border rescue activity received bigger attention. This happened because the professional agencies, which were addressed during the first project, were committed to the initiative. On the other side, the chosen topic seemed to be more manageable as the issue of cross-border movement of patients.
Aim of the subproject was to make a detailed analysis of the legal and administrative background of cross-border emergency activity with help of a professional working group, and we articulated proposals in order to terminate the existing obstacles. Hence, we wanted to achieve
- to improve the access of the citizens to emergency medical services in the border areas;
- thus, improving the quality of life of the citizens living in the border areas;
- and in the long run to contribute to more economical and more efficient operation of rescue, as well as emergency health care network through cross-border integration.
We think that the subproject was successful, since it effectively triggered a debate between the domestic competent authorities and professional bodies, as well as legislative proposals and policy recommendations were drafted in order to eliminate the existing domestic obstacles.
Presentation of the activities that were implemented within the frame of the subproject
Manager of the subproject was Enikő Hüse-Nyerges, a project manager. Working plan was prepared on 3rd of May.
Within the frame of the subproject, a study was prepared about the possibilities for organizing cross-border emergency rescue. The study included comprehensive, concrete legislative and policy proposals. The study was prepared between June and November, in 2017.
A working group with experts was set up in order to support the professional preparation of the study. The working group had 4 meetings during the duration of the project. Besides, taking into account the complex financing background of the issue, two experts were entrusted with the task to elaborate the related chapters. The relevant request was sent to the National Health Insurance Fund of Hungary on 13th of June, and we made a contract with two experts, recommended by Deputy Chief of Health, Zsolt Kiss. The two involved experts were Brigitta Paragh and Dr. László Kőrösi.
The following experts were involved within the work of the working group, except the CESCI members (Enikő Hüse-Nyerges, Dr. Norbert Jankai):
- Niertit Annamária Barbélyné, Head of Department, Department of Health Administration, Deputy Secretary of State for National Medical Tasks, Ministry of Human Capacities
- János Bathó, Head of Organization, National Ambulance Service
- Anett Blága, Administrative Adviser, Department of Health Administration, Deputy State Secretary for National Health Officers, Ministry of Human Capacities
- Pál Golopencza, Chief Medical Officer, National Ambulance Service
- Miklós Gresz, Professional Advisor, Health Care Planning Department, National Healthcare Services Center
- Anett Jova, Legal Advisor, Administrative and Legal Department, National Ambulance Service
- László Kőrösi, Deputy Head of Department, General Finance Department, National Health Insurance Fund of Hungary
- Mária Lórántfy, Regional Director, National Ambulance Service
- Brigitta Paragh, Deputy Head of Department, Department of International Relations and Legal Records, National Health Insurance Fund of Hungary.
We invited other experts to participate within the activities of the working group from the Ministry of Human Capacities, Department of EU and International Health and Social Affairs, and the experts from the Ministry of Foreign Affairs and Trade, but they did not want to participate in the joint work.
The working group had 4 meetings altogether: on 6th of July, on 13th of September, on 11th of October and on 23rd of November.
At the first meeting of the working group, critical questions of legal harmonization were identified by a narrow circle of participants (National Ambulance Service, National Health Insurance Fund of Hungary) with the help of CESCI staff. These critical issues go far beyond the health and professional fields, thus, they affect also other domains, like the issue of transport, information communications and the language competence of participants in rescue. Besides, the participants, with the representative of the National Health Insurance Fund of Hungary, thoroughly analysed the domestic and EU aspects of the funding background of health rescue activities. The participants began to identify the EU and national legislation which play relevant role in each topic, as well as they surveyed the possibilities to overcome obstacles. At the end of the meeting, they agreed on further tasks and about the scheduling.
At the second meeting, the number of participants of the working group was extended by the representative of the National Healthcare Services Center, who raised several important questions and issues in the field of cross-border rescue activity. Majority of the questions were either fully or partially answered at the meeting, but in several cases there was a need for further information gathering, legal analysis or involvement of an expert from the sector. During the second part of the meeting, the participants began to clarify the methodological questions relating to the theoretical designation of border area health care and to identify the data and information that were required by the given task.
At the beginning of the third meeting, CESCI reported on the progress of the project in the domain of clarifying professional issues and data collection. They expressed that since the previous meeting, they managed to contact with the experts of Pro-M Zrt., who assure radio services for the National Ambulance Service, as well as they contacted the company that assures ambulances and personnel staff and who answered the previously emerged questions. Subsequently, the participants with the help two experts from the Ministry of Human Capacities, National Health Office of Health Care Administration, reviewed the possibilities of extending the permits in order to carry out foreign rescue activity and they formulated their final proposal. During the second half of the meeting, the questions that were previously unanswered were clarified and the methodology for the theoretical designation of border area health care was finalised, too.
Before the fourth meeting of the working group, the comprehensive study, involving the main results of the subproject, and the draft of the bilateral agreement on cross-border emergency rescue operations were completed. Both materials were shared with the experts of the working group before the meeting. The experts sent their questions and suggestions to the prepared documents before the meeting. At the meeting, the suggestions were reviewed separately and they clarified the content of the disputed parts. On the basis of this, CESCI staff finalised the above mentioned documents.
Debated at the meetings of the working groups, legal and administrative obstacles, which hinder ambulance vehicles to cross the borders in emergency case, affect numerous areas besides health care. In order to clarify these issues, we contacted the following actors with the aim to gather information.
- We proposed to establish bilateral agreements about free crossing of non-Schengen borders. In order to clarify whether this bilateral regulation violates higher international, European regulations or not, we consulted it with the staff of the General Border Police Department of the National Police Directorate.
- We consulted about the possibilities of establishing a radio link between the ambulance and the control centre after crossing of the borders with the office of the Directorate-General for Law Enforcement of Hungarian National Police Headquarters, as well as with the employees of the Pro-M Zrt., functioning within the frames of the National Infocommunications Service Company.
- We asked the ERIX Biztosítási Alkusz és Tanácsadó Kft. about the CASCO and liability insurance of ambulance, as well as about the territorial scope and extent of liability insurance of the personnel.
- In order to formulate proposals for eliminating the identified obstacles, we contacted the Secretariat of the Nordic Council in Copenhagen, who provided assistance in order to understand the details of rescue cooperation that is implemented on the Swedish-Norwegian border, and they sent us the related basic documents for internal use.
For the spatial modelling of border areas, which was implemented within the framework of the study, an extensive data collection was needed. In order to obtain the data, we contacted the following organizations and institutions with the help of the working group members:
- Landessicherheitszentrale Burgenland GmbH (Burgenland Security Center) – Austria
- Rotes Kreuz Burgenland (Burgenland Red Cross) – Austria
- Internationale und Europäische Angelegenheiten der Sozialversicherung (Association of Austrian Social Insurance Institutions) – Austria
- Úrad pre dohľad nad zdravotnou starostlivosťou (Health Surveillance Authority) – Slovakia
- Zavod za zdravstveno zavarovanje Slovenije (Institute for Health Insurance of Slovenia) – Slovenia
- Ministrstvo za zdravje (Ministry of Health) – Slovenia
- Hrvatski zavod za hitnu medicinu (Croatian Emergency Agency) – Croatia
- Tisza ETT – in relation to Ukraine
- Transcarpathian Health Department – Ukraine
- CESCI Balkans – Serbia.
Summary of the subproject results
The starting point of the subproject
The starting point was the analysis that was implemented by CESCI in 2016, whose main findings were the followings.
- The current regulation of emergency rescue emphasizes strict territoriality. The EüM Decree no. 5/2006. (II.7.) clearly covers the territory of Hungary. On the other hand, the mentioned decree (obviously for quality assurance reasons) provides a very limited scope for the units outside the National Ambulance Service, including the ambulance services beyond the border. The EüM Decree no. 2/2004. (XI. 17.) on the register of authorization of healthcare providers, and the health professional list includes the material and personal conditions necessary for rescue operation. In order to take part in patient transport outside of the frames of the National Ambulance Service, there is need to obtain the relevant operating license from the relevant authority, but this is fully unrealistic in case of disaster situation, and it restricts the health care rights of the EU citizen who has suffered an accident.
- This is the reason that the neighbouring countries use a practice of signing bilateral agreements that relate to disaster situations. Hungary has valid agreements with all its neighbours, these agreements make details about the conditions for interventions across the border (based on commonly agreed definitions), about the scope of the competent bodies that can be involved into the assistance, about the responsibility for coordination, about the rules for the rescue teams and setting of the costs associated with the assistance.
- During the project in 2016, it became clear that regulations in the domain of traffic do not allow to use the distinctive sign by the ambulances beyond borders of a country, thus it significantly influences the manoeuvring options of these vehicles.
- Beyond the above mentioned legal obstacles, other viewpoints also have to be taken into account, like technological (radio communication), linguistic and other administrative and financial aspects, which currently appear as administrative obstacles.
- According to the surveyed experts, development of the system with cross-border rescue services is only imaginable through gradual, step by step establishment. First, it should be achieved that ambulances can freely cross the border and that the injured person can be delivered to the nearest hospital according to their citizenship. Subsequently, cross-border sharing of hospital emergency services could take place.
Contribution of the expert working group
Contribution of the working group to the final documents seemed to be very fruitful and useful, because the participating members had knowledge about the regulatory background of their own field of expertise and it significantly contributed to the exploration of the full range of existing problems and obstacles, and to the formulation of solution proposals, as well as to develop of the required methodology, to obtain the data that was needed for spatial modelling of border areas.
Besides, the preliminary concept of the CESCI was partly modified on the advice of the participating experts. According to the original idea, we wanted to take steps to enable sharing of cross-border hospital emergency services. This would mean in practice that in case of emergency rescue, the patient would not be necessarily transported to the nearest domestic hospital, but the patient would be transported to the nearest hospital, where he/she can receive appropriate health care service, even in the case when the hospital is located beyond the border. In the case of emergency care, there are no legal and funding barriers in this respect; however, equal opportunities of the injured would be violated. In order to avoid this, the experts advised that regardless of whether domestic or a health care rescue unit beyond the border provides a health care for the injured person, it should always be considered whether the patient would receive higher standard and/or faster patient care in the state of action or in a neighbouring state. However, opening of borders in this specific issue would generate capacity and financial risks because of the expected increase in emergency cases. The volume of the expected increase is not known, yet. Therefore, the problem goes far beyond the scope of this project and study; consequently, we only dealt tangentially with this specific topic.
The main findings and suggestions of the study
The expert study can be divided into three major parts:
- In the first part of the document, we provide a brief overview about the justification of the cross-border movement of ambulances, as well as we introduce the related European Union processes. Then, we give a theoretical introduction into the basic elements of the emergency care services, and we describe the domestic emergency system and the emergency system of the neighbouring states, taking particular attention to factors that affect cross-border cooperation.
- In the second, most prominent part of the document we analysed the conditions of implementing cross-border emergency rescue through thematic approach, then we formulated legal and policy recommendations. The following topics were processed in this chapter:
- the conditions for crossing the border: Schengen, non-Schengen internal borders and external borders
- operating licenses: material and personal criteria
- use of distinctive signs and their criteria
- administrative-technical issues: liability and vehicle insurance, fuelling, travel notes, etc.
- professional cross-border cooperation from rescue alert to patient hospitalization
- communication: radio contacts, linguistic obstacles
- financial questions: financial aspects of rescue activity and emergency hospital care.
The formulated legal proposals and policy recommendations in the document were separately summarized on European, bilateral and national level, we reviewed the priorities of the recommendations, time horizon for implementation and we formulated a series of actions that aimed practical implementation.
A) We made a proposal at the European level to define the concept of cross-border rescue, mutual acceptance of operational and distinguishing signs beyond the border (similar to the Directive No. 2011/24). The applicability of the Directive would be based on the condition that the involved member states voluntarily settle the terms and conditions of cross-border cooperation.
B) We recommend to regulate the following aspects of cross-border rescue through bilateral agreement:
- cross-border zones that might be included within cross-border rescue activity;
- free movement of rescue vehicles using distinctive sign within non-Schengen borders;
- the type, minimum conditions and competences of the rescue team that ca be sent across the borders;
- the sequence of alarm and command of the rescue unit beyond the borders;
- details of the cooperation between domestic competent units (ambulances, dispatch centre, etc.) and rescue units beyond the borders;
- the sequence of transferring the patient to the domestic rescue unit or transporting the patient into the hospital.
- protection and support for the rescue units beyond the border;
- setting up a translation service that helps the rescue.
C) Depending on the new provisions at European and bilateral level, in some cases it is necessary to implement amendments within the related domestic legislation. The new proposed legislations will affect the content of the following domestic provisions:
- content extension of the Decree No. 96/2003. (VII. 15.) on the general conditions for providing health care services and on provider licensing relating to the mutual acceptance of operating licenses;
- modification of the Decree No.5/2006. (II.7.) EüM on Emergency Rescue Services relating to personal and material conditions, alarm and command of rescue units beyond the borders, as well as transferring and transporting the patient to hospital;
- content extension of the Decree No 12/2007. (III.13.) IMR relating to distinguishing signs;
- modification of the Decree No. 41/2004. (IV. 7.) GKM relating to distinguishing signs.
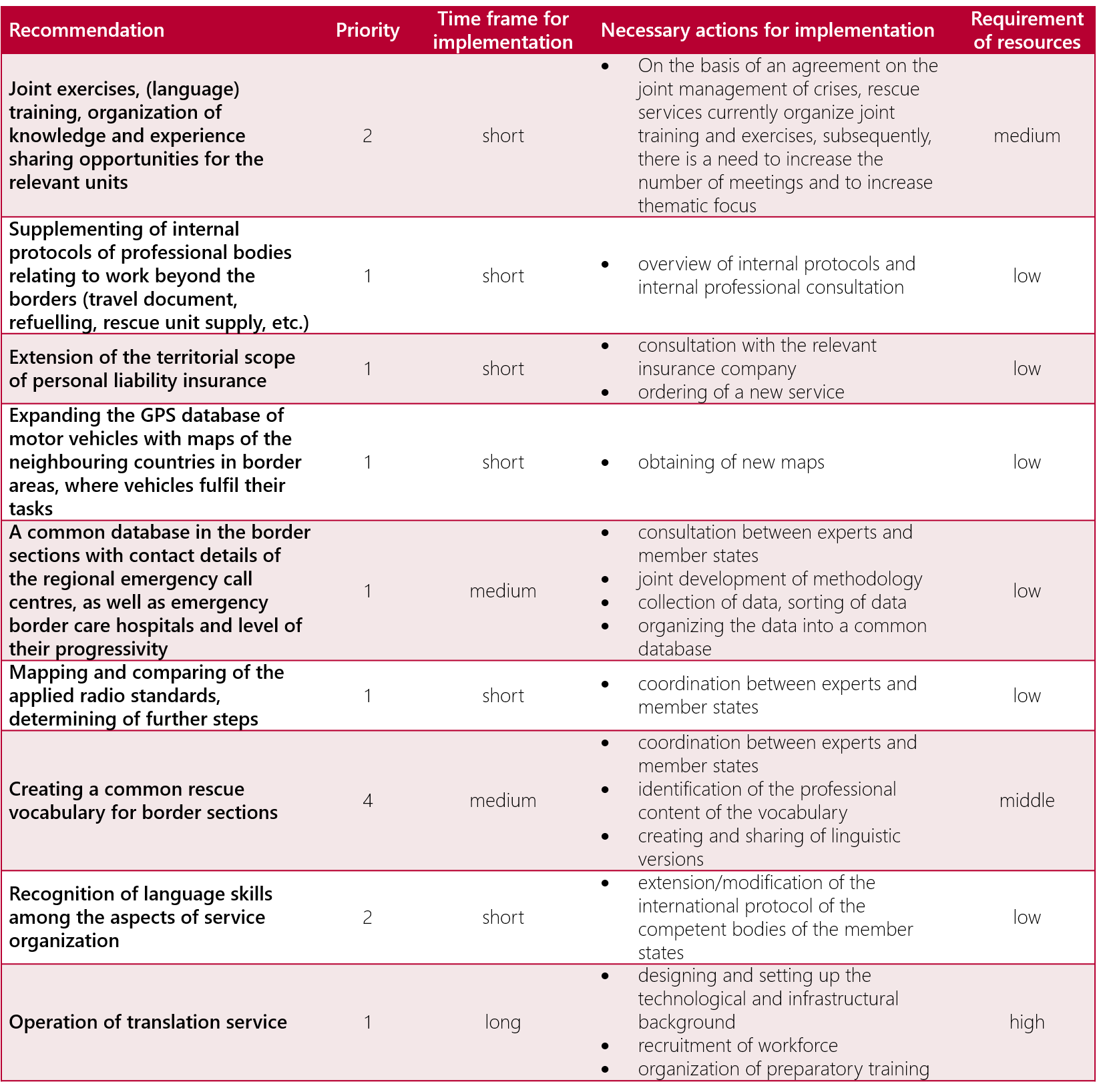
D) Policy recommendations, priority of the recommendations, or the necessary action steps, their time horizon and costs for implementation
It became clear during the project that modification of the legal instruments alone is not enough in order to establish the conditions for cross-border emergency rescue activity, hence formulation of policy recommendations at European and/or bilateral level is necessary for each concerned topic.
Table 1.: Recommendations for the European Union
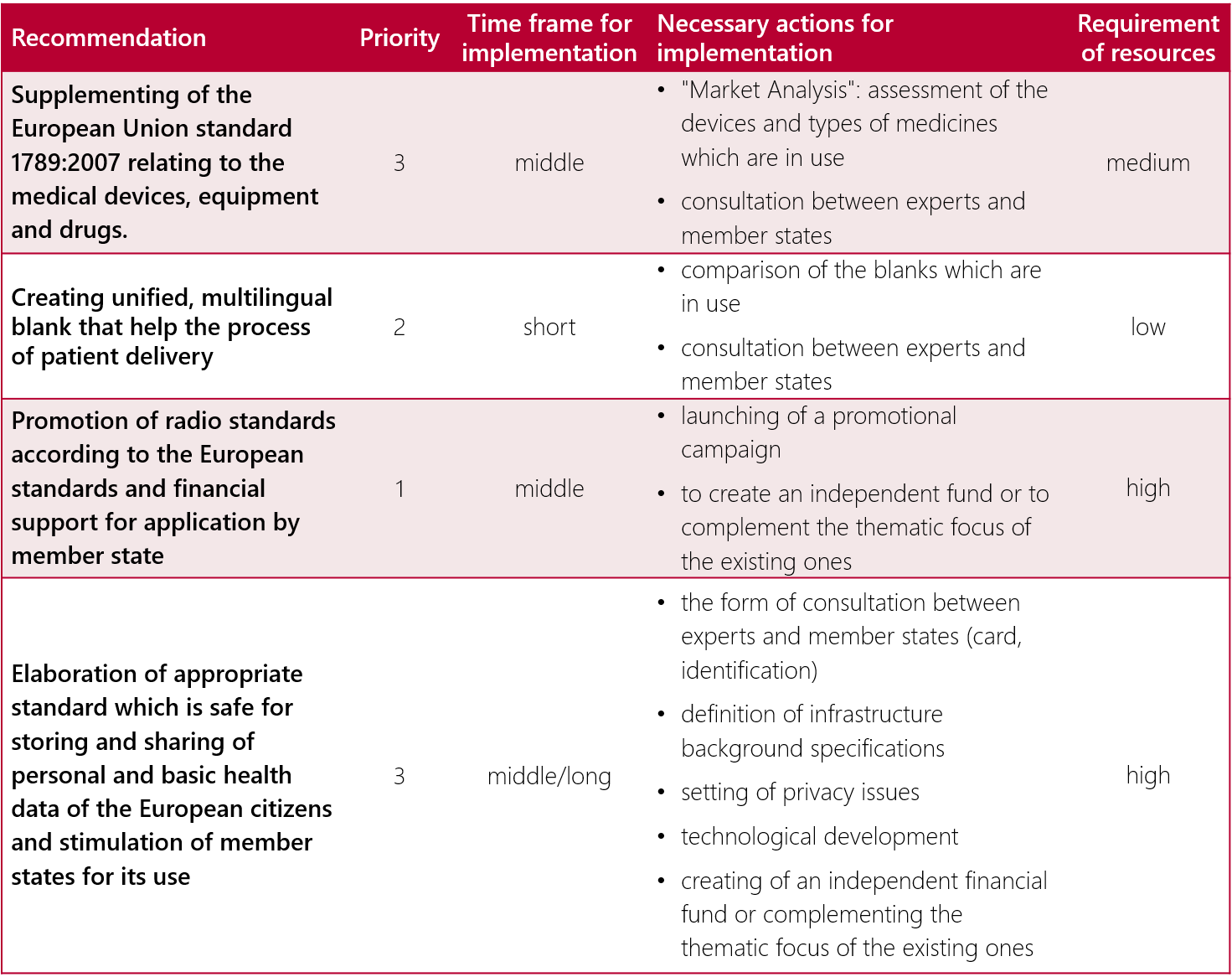
Table 2.: National and/or bilateral policy recommendations
In the third part of the study, we modelled and analysed the territorial aspects and potentials of cross-border rescue and emergency hospital care at the theoretical level.
- 50 km from the border crossing point, based on the methodology that is used in the Hungarian Emergency Rescue system, we have determined the area of 50 minutes availability, where it is worth to explore the possibility of allowing cross-border rescue activity. According to the participating experts within the project, this is the area, where the injured person can get access to appropriate on-site or hospital care by the rescue units of the neighbouring state.
- During the analysis of the territorial pattern of rescue services at the border, we took into account the location of the rescue stations and border crossing points, as well as time factor which is related to the arrival of the rescue unit to the given location (15 and 30 minute zones).
- Within the frame of the project, we had only limited scope to deal with legal and administrative aspects of cross-border emergency care and its possibilities, we wanted to point out the potentials of cross-border cooperation. This chart illustrates emergency hospitals within border area that are identified within the project; as well as it attempts to visualize the spectrum of benefits offered by the given institutions.
This and elimination of all the other obstacles clearly require not only the effective and high-level cross-border cooperation among wide range of professional organizations, but there is a need for co-operation and problem-solving intention at high political level between neighbouring member states; however, we currently experience shortcomings in this domain.
Fulfilment of the identified indicators of the subproject
|
Title of the indicator |
Required |
Fulfillment |
| Ad-hoc health care working group |
1 working group |
1 working group |
| Number of meetings of the health care working group |
4 meetings |
4 meetings |
| Number of invited experts into the ad-hoc working group |
10 persons |
12 persons |
| A regulatory and policy document on cross-border transport of patient |
1 regulatory and policy document |
1 regulatory and policy document |
Possibilities for continuing the subproject
Based on the formulated proposals and the identified difficulties, the following continuation option is conceivable.
1) In order to organize a cross-border emergency rescue, we recommend to address and involve the competent authorities of the neighbouring countries, hence exploring the opinions of the authorities on existing policy orientations and developments in the neighbouring countries. This could allow the formulation and finalization of bilateral proposals for legislative harmonization.
2) The other segment of cross-border emergency cooperation is embodied by the emergency hospital care. Nevertheless, cross-border sharing of hospital health care services carries unknown degree of risk, which is unacceptable for the member states. In order to handle the situation, it would be necessary to make a detailed analysis of the issue and to quantify the volume and consequences of potential cross-border patient movement.